BY ANISH KOKA
The European Medicines Agency decided on July 19, 2021 that myocarditis and pericarditis be added to the list of adverse effects of both messenger RNA (mRNA) based vaccines (BNT162b2 [Pfizer-BioNTech] and mrna-1273 [Moderna]) against COVID-19. This advice was based on numerous reports of myocarditis that followed a clinical pattern that strongly suggested a causal link between these particular vaccines and myocarditis/pericarditis. The adverse events that appeared to be predominantly in young men typically occurred within a week after injection, and were clustered after the second dose of the vaccine series. A recent national database from France sheds some light on the approximate rates of mrna vaccine related myocarditis.
Between May 12, 2021 and October 31, 2021 within a population of 32 million persons aged 12-50 years, 21 million first doses of the BNT162b2 (Pfizer) vaccine and 2.86 million first doses of the mrna-1273 (Moderna) vaccine. In the same period, 1612 cases of myocarditis and 1613 cases of pericarditis with myocarditis were recorded in France. Compared to matched control subjects, the risk of myocarditis was markedly increased after 1st and 2nd doses of the vaccine. For the Pfizer vaccine, the odds of myocarditis were 1.8 times the expected background rate for the 1st dose and 8 times the expected background rate for the 2nd dose. The Moderna vaccine, which delivers about three times the dose of the Pfizer vaccine has an even higher risk of myocarditis — a stunning 30 times the expected background rate after the second dose. A prior history of myocarditis was associated with an odds-ratio of 160.
Odds ratios can be challenging to translate into a real sense of risk especially when dealing the a clinical diagnosis that is as rare as myocarditis is. A clinically busy cardiologist may see one case a year if they’re lucky, so a therapy that doubles the risk of myocarditis may seem a lot more scary than it actually is. In the case of this French database, a helpful supplemental table shows the risk of myocarditis is highest after a second dose of the Moderna vaccine in males aged 18-24 year old at a rate of 1/5900. The next most at risk group is 25-29 year old men with a rate of 1/9400.
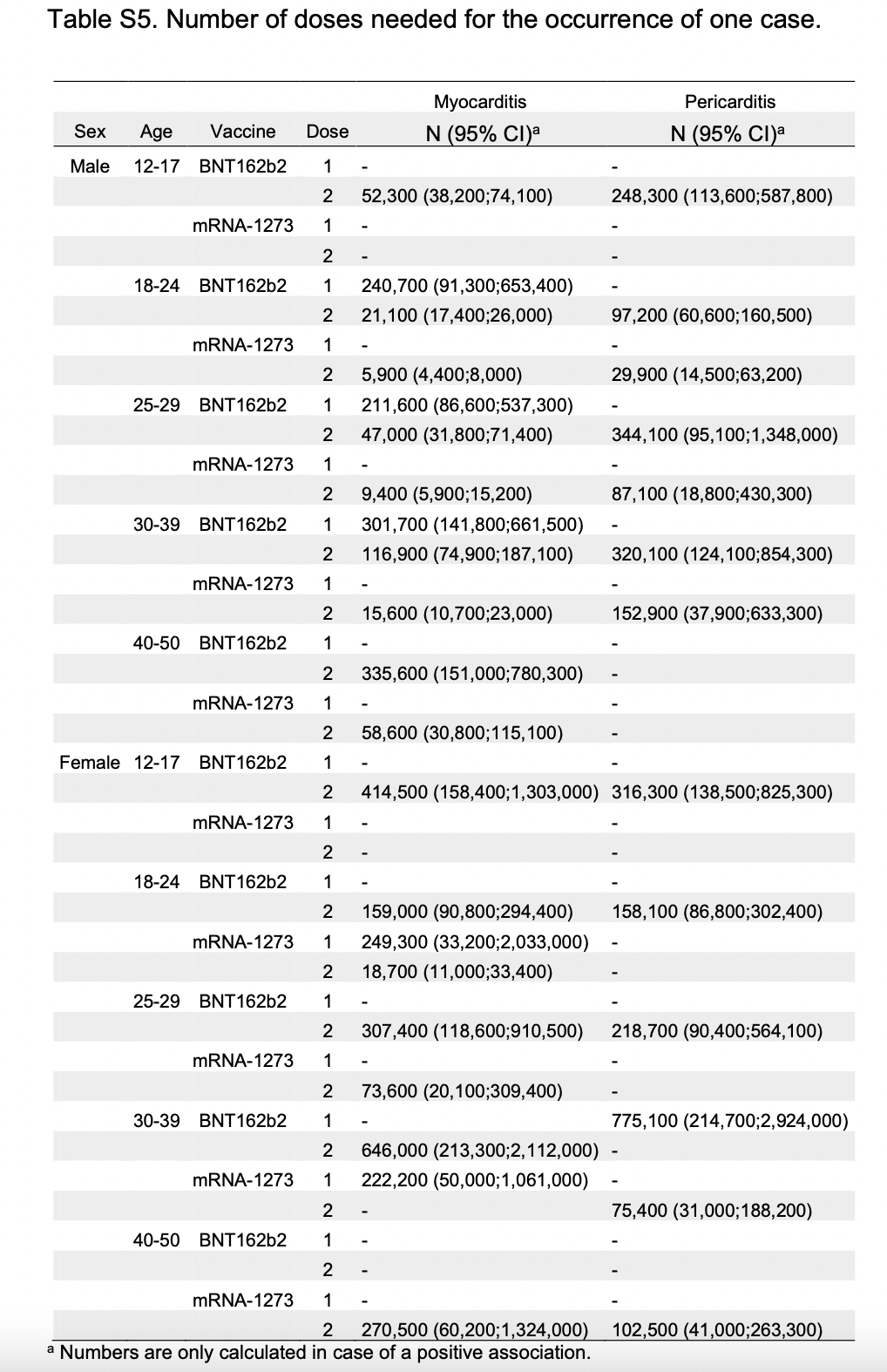
Clearly, women have higher rates of myocarditis compared to background as well, but like most other databases to date, the rate of myocarditis is lower relative to men. The highest risk of myocarditis is in women aged 18-24 after the second dose of the Moderna vaccine at a rate of ~ 1/18,700.
The limitations to this study relate to how the diagnosis of myocarditis was made. Cases of myocarditis in this study were based solely on diagnosis codes associated with hospital admissions. This means the estimates here miss cases of myocarditis that never made it to the hospital, but also may overcount hospital admissions mislabeled as myocarditis.
Scientifically, there is no doubting the link between mrna vaccines and myocarditis. Even the CDC director that spent much of 2021 denying this possibility must now know this whether she is allowed to publicly say so or not. Even if one was to buy the party line that the mrna vaccines are beneficial in every age group for time immemorial, it would seem to be a matter of basic ethics to inform the public that one of the mrna vaccines (Moderna) has consistently been noted to have significantly higher rates of a serious adverse event in a particular demographic (young men). I would hope that, at least, most cardiologists would be saying this, but a relatively recent (February 2022) perspective in the Journal of the American College of Cardiology that I can only assume is meant as guidance for Cardiologists brings up the issue in the context of the potential declining efficacy of vaccines related to new variant, only to dismiss it by referencing a CDC retrospective study that suggests fewer deaths in those vaccinated and boosted in the 18-49 age group.
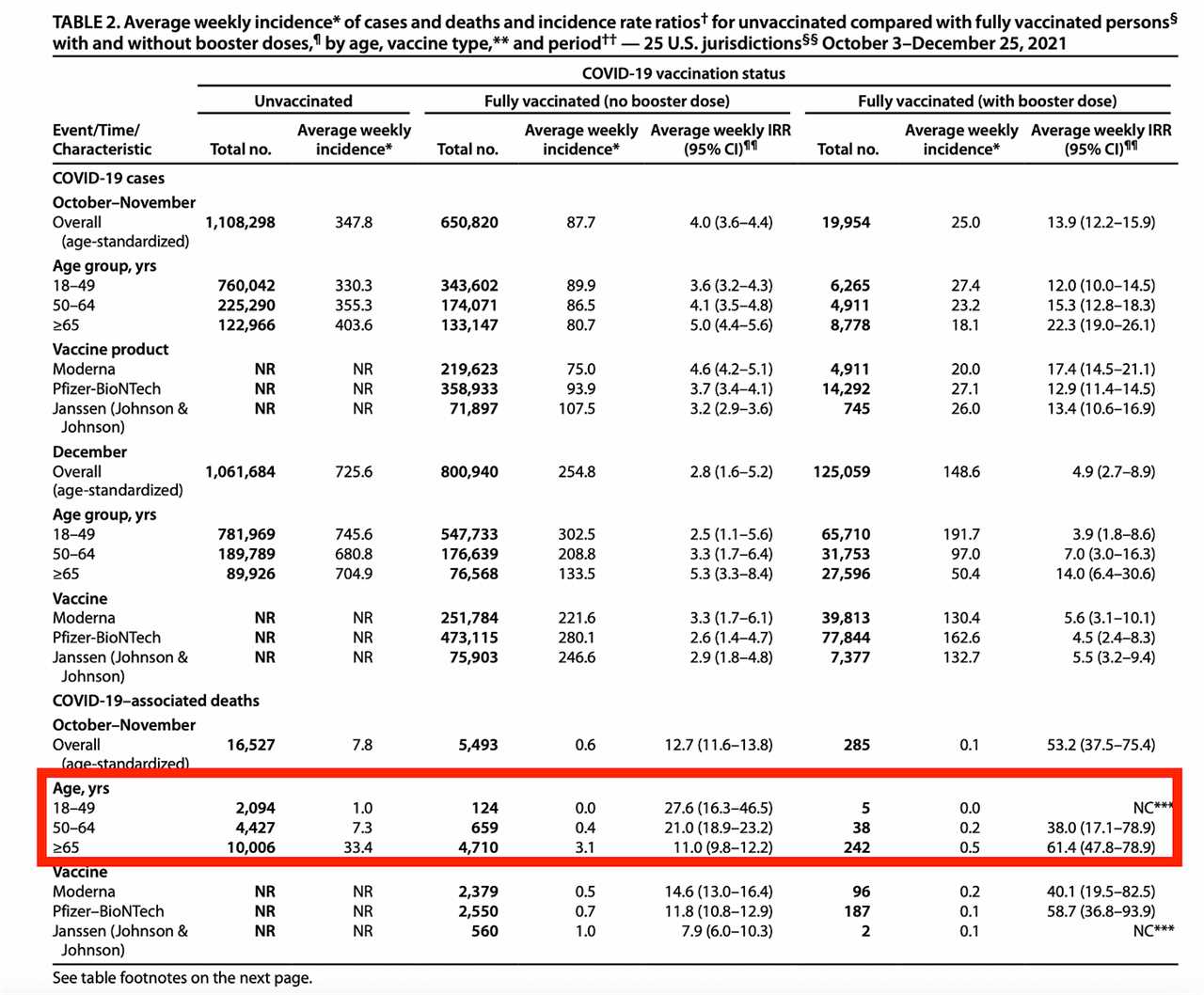
There are a number of problems using this reference. To start, given the massive COVID age risk gradient, the vast majority of deaths in an 18-49 year old category cluster towards the top of the category. Its not clear why the CDC, or the ACC think that a distribution of deaths between ages 18-49 that is clearly not going to be evenly distributed based on what we know of the underlying disease has much relevance when discussing a serious adverse event of vaccines that relates to 18-24 year olds. The other major problem is that there isn’t even an attempt made in this CDC report to adjust for underlying differences between the vaccinated and unvaccinated individuals, which prompts these words in the CDC publication:
…this ecological study lacked multivariable adjustments, and causality could not be determined. Possible differences in testing, infection-derived immunity, waning of vaccine-derived immunity, or prevention behaviors by age and vaccination status might partly explain differences in rates between groups.
Another CDC reference related to booster efficacy during omicron predominance suffers from the same fundamental problem – the age grouping used to evaluate the outcome of choice in this study (ED and urgent care encounters) is once again 18-49 years old, and once again, the retrospective nature of the study leaves open the very real possibility that efficacy estimates are effected by unmeasured and residual confounding.
So we now have numerous reports over the course of a year and a half from various different databases that started with an Israeli study that first reported rates of myocarditis between 1/3000-1/6000 in young men in April of 2021, with a clear signal that the Moderna vaccine’s higher dose may be leading to markedly higher rates of myocarditis than its Pfizer counterpart. Yet, US officials are inexplicably silent on the matter despite the fact Sweden, Denmark, Finland and Iceland have all paused the use of the Moderna vaccine in young people in the Fall of 2021. While I understand the fear public health officials may have about undermining vaccine confidence, this type of politics only undermines global vaccine confidence further. It should also cast a significant shadow on vaccine mandates that now serve as barriers for young people at places of work and school.
I have to make the obligatory post-script here that I oversaw the administration of hundred of mrna vaccines starting in March of 2021 in my cardiology clinic. The vaccine efficacy data for the original data was from thousands of patients and I certainly felt given the devastation wreaked on many of my patients in 2020 that the vaccines were the best chance of avoiding morbidity and mortality. The process to get the vaccines from the city department of health was a somewhat arduous 3 month process, and once the vaccines were on hand, there were daily reporting requirements that I dutifully performed for the many months we were administering vaccines. To accommodate the rush of patients, employees, volunteers, and conscripted children worked multiple weekends to administer the vaccines. So I’m especially disgusted by medical colleagues who label any concerns registered about vaccine adverse events as “anti-vaxx”. Registering concern over a vaccine adverse event does not make doctors or patients “anti-vaxx”.
Anish Koka is a Cardiologist.
-----------------------------------------
By: Ryan Bose-Roy
Title: Vaccine Myocarditis Update
Sourced From: thehealthcareblog.com/blog/2022/09/07/vaccine-myocarditis-update/
Published Date: Wed, 07 Sep 2022 14:15:07 +0000
Read More
Did you miss our previous article...
https://naturesmart.us/health/putting-the-e-in-dna
 HealthWellnessFitnessBeautyVideosRecipesPrivacy PolicyTerms And Conditions
HealthWellnessFitnessBeautyVideosRecipesPrivacy PolicyTerms And Conditions
