BY ANISH KOKA
Apparently, the US Food and Drug Administration (FDA), that has long been charged with the safety and efficacy of drugs and devices now also controls who can prescribe drugs.
I was under the mistaken impression that in our highly rule based society you would need to pass a law to allow that to happen. Passing laws , of course, can be a long, messy, process that involves having to convince constituencies, and ruling by executive order is just way more efficient apparently.
So by decree of the FDA patients can now get Paxlovid, an anti-viral for the virus that causes COVID19, “directly from their state licensed pharmacist” if they so choose. Apparently, someone in government decided that there wasn’t enough Paxlovid being prescribed, and the major rate limiting step for many patients is not having access to a provider to prescribe the drug. I have to say provider now because physicians long ago lost the monopoly they enjoyed for prescribing medications to nurses with advanced degrees and physician assistants. The next obvious step is to cut out the ‘clinicians’ completely by allowing patients to get medications from a pharmacist without a prescription.
Its interesting because I’ve struggled with quite a few Paxlovid requests recently. About 5 weeks ago a long time elderly patient of mine with a history of coronary disease and a stroke called me during dinner because he had just contracted COVID. He had been more lethargic and a concerned wife took him to the ER, where he was found to be COVID positive. He was vaccinated and boosted, and we went back and forth about the different options. We finally decided to go ahead with Paxlovid. Paxlovid has a long list of interactions with a variety of drugs that make it unsuitable for many, but luckily he was only on a cholesterol lowering medication that we could hold for some time. Problem solved. So I thought.
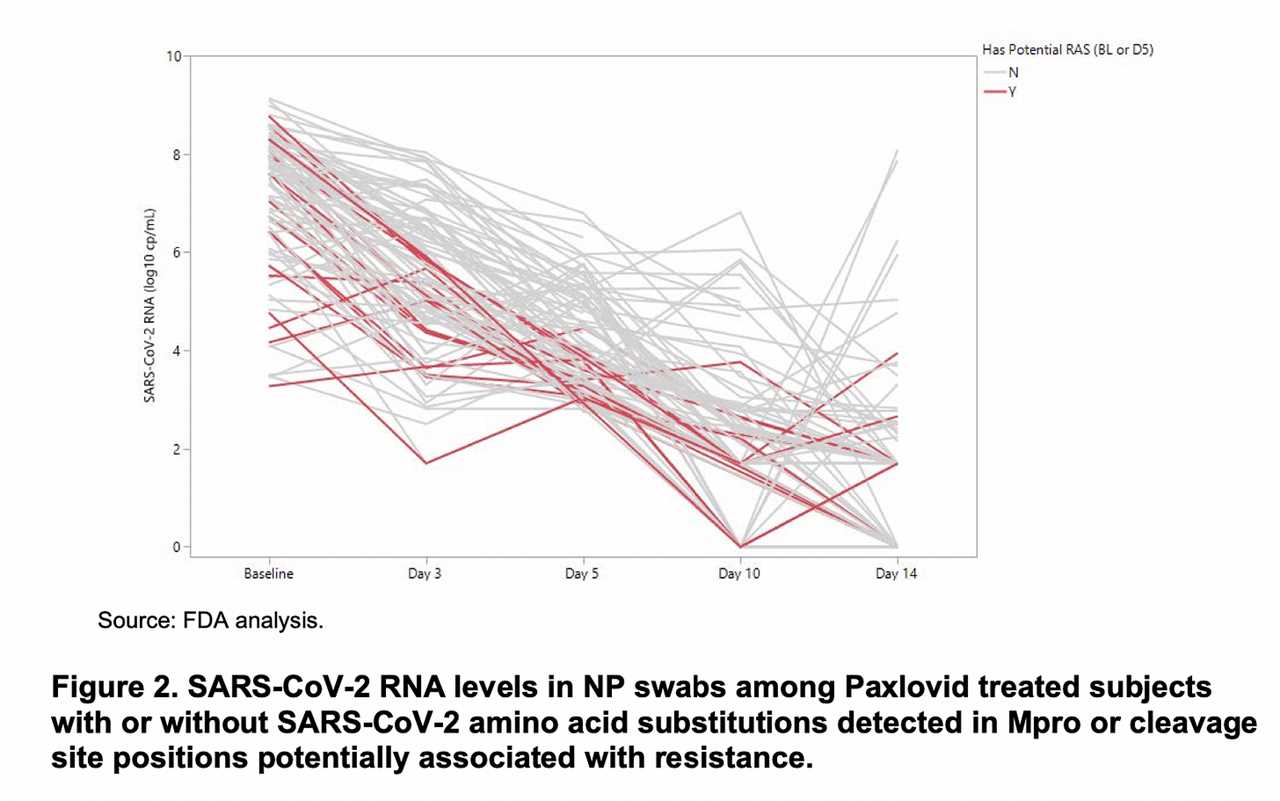
Six days later I got another panicked call, this time from an ER. Mr. X had been doing just fine until he starting having fevers and chills. He had finished his Paxlovid course the day before. Back in the hospital, testing revealed a positive covid antigen test. Luckily this hospital stay was just a 36 hour stay. No other infectious sources were found, though a bacterial antibiotic was started out of ‘caution’. Its hard to know exactly what happened but one possibility is a phenomenon known as COVID rebound – where the virus surges for unclear reasons after completion of the anti-viral course. Interestingly, this was an adverse event that the FDA and Pfizer, the maker of Paxlovid, were aware of. We know this because of a chart found in the FDA emergency use authorization documents that was not available in the peer reviewed paper that appeared in the New England journal of medicine.
Medicine is a complicated business and one of the factors I discussed with the patient and his wife when prescribing Paxlovid was the fact that he wasn’t very well represented in the trial that demonstrated a benefit for Paxlovid in treating COVID19. The impressive reduction in severe disease that Paxlovid demonstrated in the Table below is based on an earlier Sars-COV2 variant that infected unvaccinated individuals.
There is already plenty of evidence from the historical record that prior infections are protective against progression to severe disease from future infections (This is the literal basis for vaccination), and there is every reason to also believe that prior vaccinations may be protective as well. This is exactly what the Paxlovid trials that lead to FDA approval demonstrated as well. (Figure 1)
Patients in the trial with positive serology for the virus (i.e. those who had recovered from COVID) had a markedly smaller benefit with Paxlovid use. Ninety-eight percent of the patients who received a placebo in the trial did not progress to severe disease. The implications here are immense. Given that contact with Sars-COV2 is an inevitability for all the future offspring of Nick Cannon and Elon Musk, I could become a very rich man marketing my special version of camel urine as a treatment for COVID.
So there was every reason to believe at the time I was prescribing Paxlovid that I was exposing my patient to the adverse events of a drug with little to no benefit. Sure enough, two weeks later Pfizer released updated results of a study of Paxlovid use in patients that were vaccinated and found the reduction in hospitalization and death to be non-significant. From a sample of 721 vaccinated adults with at least one risk factor for progression to severe COVID, 3/361 who received Paxlovid progressed to severe COVID compared to 7/360 patients that received placebo. The statistically insignificant results don’t mean there was no benefit. Given that the drug inhibits viral replication, and the clinical context it was used in, the fewer number of patients who ended up severely ill who were given Paxlovid is unlikely to be a statistical fluke, but it does indicate any benefit of Paxlovid in a high risk, vaccinated population is very small. This is actually good news. Whether it be the newer variants circulating are more benign, or that vaccination against the original Sars-COV2 variant is providing robust protection, these results strongly suggest that doing nothing leads to a good result the vast majority of the time. The Pfizer press release differs a bit from this conclusion. Albert Bourla, CEO of Pfizer summarized the data in this fashion:
“Results from our Phase 2/3 EPIC-HR and EPIC-SR studies, as well as post-authorization experience, support the efficacy and safety profile for PAXLOVID in the treatment of mild-to-moderate COVID-19 patients with at least one risk factor for progressing to severe COVID-19, regardless of vaccination status,”
He isn’t technically wrong, but he is choosing to downplay the likely minimal benefit of the drug he manufactures for most people. He’s doing his job – which is to pump up the parts of the Paxlovid data that will result in more prescriptions of his drug. Later on in the press release we find this nugget :
The results from these additional analyses are not expected to impact Pfizer’s full-year 2022 revenue guidance.
Since this data has come out, I’ve received a number of other calls from patients who tested positive for COVID. Most of the calls are from young vaccinated patients that I wouldn’t have ever thought were appropriate for Paxlovid. Some have been from higher risk, but still vaccinated patients. The messages are, interestingly all about the same. “Patient tested positive for COVID, wants Paxlovid”. None of the subsequent conversations I have had have resulted in me prescribing Paxlovid. It turns out patients aren’t really excited about getting medications. The vast majority just want some reassurance from a professional that it’s ok to not take a drug.
That this is the context the FDA decided to roll out “pharmacist Paxlovid prescribing” says a lot more about what’s going on at the FDA than what’s going on with COVID and the therapies for COVID.
Here’s hoping the Pharmacists are a little more plugged in than the FDA is.
Anish Koka is a Cardiologist.
-----------------------------------------
By: Ryan Bose-Roy
Title: Pharmacists Can Now Prescribe Paxlovid. Good idea?
Sourced From: thehealthcareblog.com/blog/2022/08/22/pharmacists-can-now-prescribe-paxlovid-good-idea/
Published Date: Mon, 22 Aug 2022 12:51:38 +0000
Read More
Did you miss our previous article...
https://naturesmart.us/health/rural-america-is-a-fertile-field-for-digital-health
 HealthWellnessFitnessBeautyVideosRecipesPrivacy PolicyTerms And Conditions
HealthWellnessFitnessBeautyVideosRecipesPrivacy PolicyTerms And Conditions
